Code green

Hospitals aren’t just another building; they are a processing facility in which lives are being saved daily – this requires reliability and energy. So, can we please stop bundling them in with other building types when it comes to talking about green buildings? James Moyes, Simon Witts, M.AIRAH, and Broden Kay are asking this pointed question.
Take one look through LinkedIn and you’re more than likely going to see several articles or posts talking about the environment. It might be some wonderous new “Green building”, a state-of-the-art latest technology or a call for action.
This is a direction we all know must happen and it appears the government is finally waking up and doing something. Great.
From an energy perspective a kWh of gas is about four times cleaner than a kWh of electricity in terms of CO2 equivalent in Victoria
First, do no harm is the first principle of medicine, clinical care is the priority. Hospitals present a significant challenge in the all-electrification process. Most of the articles and thought pieces we see on all-electric hospitals are, in the main, northern hemisphere-centric, with a heating-led climate and focus totally on system and running costs compared to a “traditional” fossil-fuelled design. If there is a mandated requirement, then cost becomes irrelevant.
Very few articles even acknowledge the fact that the systems they are discussing are an integral part of a clinical delivery system. The focus here needs to be on healthcare first and foremost; these are not commercial offices for big corporates.
There is a whole suite of literature out there that highlights all the benefits of electrification of buildings. Electric buildings use less gas, therefore problem solved. Easy, next. Except we’re not in Greenland. The Australian grid on average produces more than three times the amount of CO2 per kWh/capita compared with the rest of the world.
Once the grid catches up, then electrification is good. Now, and especially in Victoria and New South Wales, the grid can in no way be classified as green. In fact, from an energy perspective, a kWh of gas is about four times cleaner than a kWh of electricity in terms of CO2 equivalent in Victoria.
We’re heading in the right direction, it is improving, but not quick enough. In 2021, 24 percent of Australia’s electrical generation was renewable, so it’s difficult to accept for companies and government entities to say, “We will solve our fossil fuel issues by buying green power” because there isn’t enough to go round. If everyone signed up, 74 per cent of them will be either disappointed or misled by their power providers.
So, what does electrification of buildings have to do with clinical care?
The prime objective of a healthcare facility is to improve the health and well-being of the occupants; the engineering services within a healthcare facility are a fundamental part of this process. Patients and staff have a right to expect that engineering systems and equipment will be designed, installed, operated, and maintained to standards that will enable them to function efficiently, reliably, and safely.
The unique nature of healthcare premises – and the dependency of patients on the provision of effective and efficient engineering services – requires that engineering systems must be resilient to maintain the continuity of health services and ensure the ongoing safety of patients, visitors, and staff. Multiple fuel sources give these facilities clinical resilience.
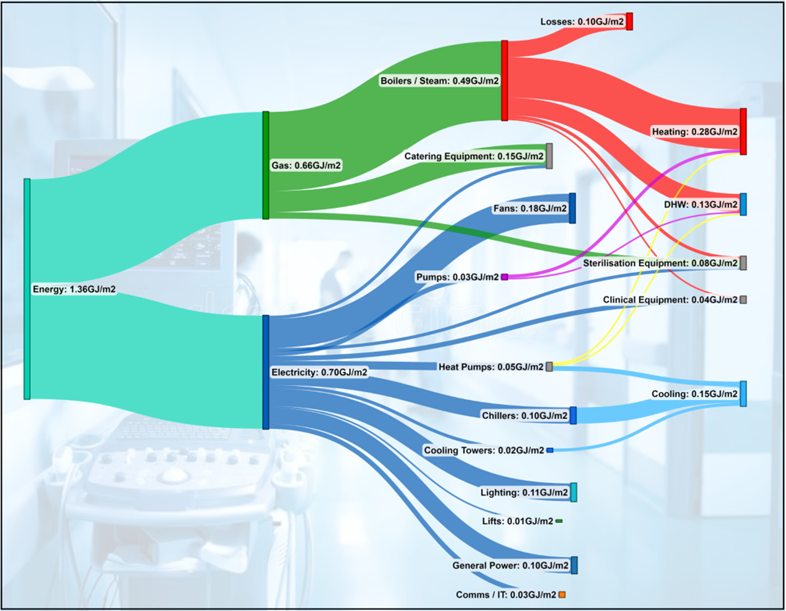
Hospitals are not low energy users. In fact, the average energy density of a hospital in Victoria is 1.4GJ/m2 per year. To put that in perspective, a 5 star premium-grade commercial office building in Melbourne would be around 0.35GJ/m2.
Now, this isn’t to say we should not be trying to reduce energy consumption. There is no excuse for poor or wasteful design. However, we should not be trying to artificially reduce energy consumption to the detriment of patient care.
So where does all the energy go in a modern acute hospital?
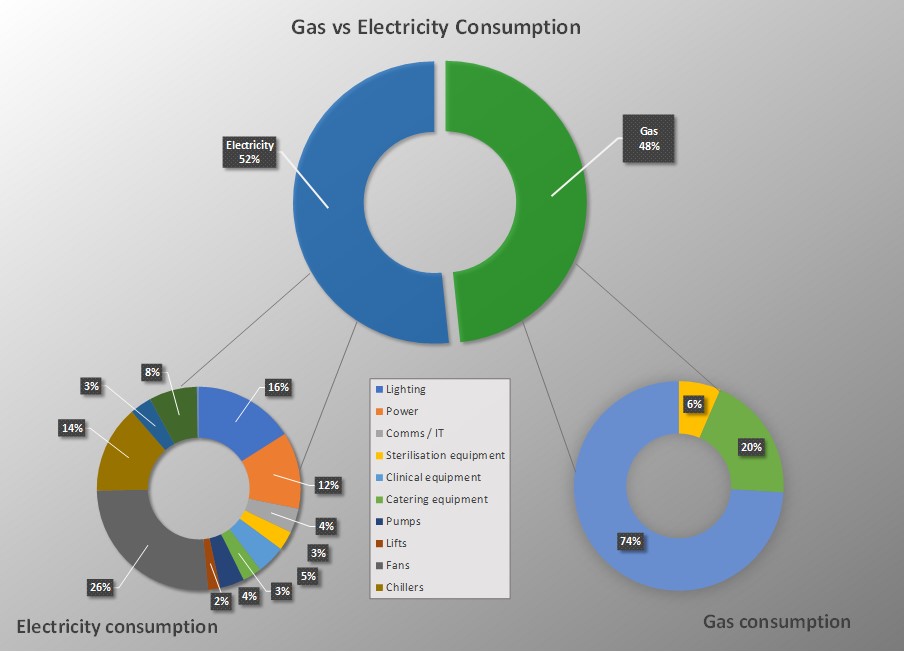
The energy consumed in a hospital is roughly the same across all hospitals in Victoria and is close enough to a 50/50 split between gas and electricity.
If we look at how the gas is consumed, 73 per cent is burned heating boilers and steam-generation equipment, 20 per cent is used directly for catering and 7 per cent is used directly by sterile services departments.
The electricity is split as we would expect – lighting, general power, equipment and HVAC equipment.
If we focus in on the energy usage by HVAC systems, this typically accounts for a whopping 65 per cent of the total energy consumed by a hospital. This isn’t too surprising when considering the amount of ventilation and associated treatment of this air but is still a very large proportion.
Well, what happens when this natural gas supply gets removed?
For new, small-to-medium-sized, one-off healthcare buildings, with a mandate in a brief, it is relatively simple to design and construct an all-electric facility. Some minor challenges within the BCA (Building Code of Australia) that limit the amount of electric reheat allowed within buildings, and limitations on the size of electric water heaters (NCC Vol 1 J5.9) exist; however, these limitations are simply regulation, so can be changed. There are no engineering showstoppers; everything is achievable.
What are the options for de-gassing an acute facility in the CBD, with minimal risk to patient care or clinical service delivery?
The biggest challenge facing new large facilities and existing hospitals is their energy density. When compared to commercial offices, a hospital can require three to four times the energy per square metre. As such, the opportunity for onsite renewable generation is extremely limited. This problem is compounded by the fact that most of our hospitals in Australia are landlocked, and the roofs are heavily loaded with engineering services necessary to support the clinical functions – and even helipads for the major facilities.
Legacy issues must be considered – very few hospitals are built from a greenfield site. They are often part of wider campuses, and the larger hospital campuses are based around a central energy plant, from which services such as steam, chilled water and heating hot water are distributed. It is not uncommon on many hospital campuses to find buildings and plantrooms that are 40 to 50 years old and still vital to the function of the facility. Careful consideration is needed when deciding whether to maintain and electrify these nodes, or to decentralise the energy generation around campus to achieve the all-electric solution. Whichever option is chosen, significant planning, design and implementation will be required to ensure that there is no impact on the clinical functional or system resilience, and this doesn’t happen overnight.
What are the effects on maximum demand if we swap out gas for electricity?
Removing natural gas from a hospital necessitates an increase in electrical demand – the systems are still required at the end of the day.
By breaking down the gas demand into their respective systems, we can calculate what the corresponding electrical load per system would be. For example, the heating portion of the boilers would be replaced by a heat pump. Taking into account the losses of the boiler and the coefficient of performance of a typical heat pump, we get the corresponding electrical demand to replace the gas-fired system.
It is important to review each system individually, because the respective electrical-based technology would have a different electrical-to-heat energy conversion, which affects the overall demand.
Taking the summation of these systems, we can calculate roughly a 30 to 40 per cent increase in electrical energy consumed. Obviously, this will vary on a case-by-case basis, but generally this is a consistent figure for modern hospitals around the world.
In terms of a maximum demand, we have to consider the existing peaks and when the additional load will occur. Incidentally, when these figures are run through an IES model, it shows that the increased maximum demand is also around 40 percent also, but the peak demand now occurs in winter, not summer.
What are the effects on the local infrastructure?
The Victorian grid is already struggling with capacity in the CBD. Every project nowadays seems to require upgrades to local infrastructure for even the smallest of increases. An increase of 25 percent per site is therefore no mean feat, especially for existing category 1 hospitals.
For our example hospital, the maximum demand would increase from 9.5MVA to around 13.5MVA. Not only would this mean multiple and expensive substation upgrades but would also require careful planning to ensure the continuity of supply. Having one of the two mains supplies offline for an extended period is a significant risk to the clinical services – how will this be managed?
The above is also assuming that there are no further upgrades required outside of the site to support this. Often, this is not the case. So, who is going to pay for these upgrades?
This is not to say it cannot be achieved, but the planning and implementation goes far beyond the typical upgrades for a commercial premises.
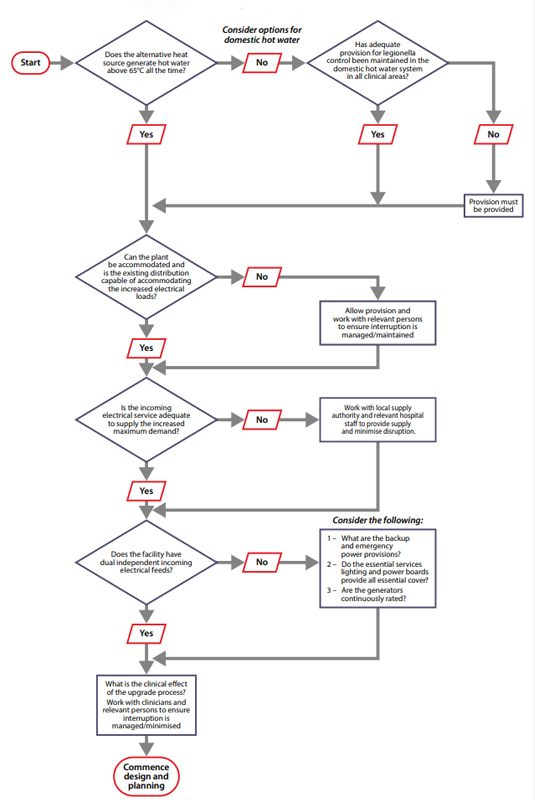
The flowchart shown opposite displays a few things to consider during the planning and implementation of removing natural gas from a hospital, starting with heat pump systems.
This article appears in Ecolibrium’s August-September 2022 edition
View the archive of previous editions





Latest edition
See everything from the latest edition of Ecolibrium, AIRAH’s official journal.