Striking a balance: planning and implementation considerations for natural gas removal in hospitals

Abstract
This paper examines the challenges associated with removing natural gas from hospitals and transitioning to all-electric systems. It emphasises the unique energy requirements of hospitals and the need to prioritise patient care and safety over energy efficiency. The study explores the impact of electrification on healthcare operations, energy consumption, and local infrastructure. It highlights the importance of careful planning and implementation to ensure a smooth transition and maintain system resilience. The findings provide valuable insights into the considerations and steps involved in removing natural gas from hospitals.
1. Introduction
This paper delves into the pressing issue of electrification in healthcare facilities, with a particular emphasis on the challenges faced in removing natural gas from existing hospitals. Hospitals are critical in saving lives, and their energy needs differ from other building types. While there is a growing trend (rightly so) towards green buildings and the adoption of state-of-the-art technologies, it is essential not to underestimate the engineering difficulties associated and maintain a priority towards prioritising healthcare delivery.
This paper highlights the need for a comprehensive understanding of the unique requirements and constraints of healthcare environments when compared to commercial buildings, challenging the predominant literature that primarily focuses on energy efficiency and cost savings. Additionally, the paper examines the specific context of Australia, where the grid’s higher CO2-e emissions per capita present additional complexities in the pursuit of reducing greenhouse gas emissions through electrification. Through this analysis, the aim is to contribute to a more holistic and healthcare-centric approach to electrification in healthcare facilities through raising awareness.
2. Hospitals don’t turn off
Hospitals are, by their very nature, occupied 24/7. Their primary function is to improve the health and well-being of the occupants. Engineering services are a fundamental part of this. It is no secret that the occupants are more reliant than the general public to ensure they leave healthier than they enter.
Historically hospitals have also been a place of last resort. They are a centre for gathering in the face of adversity due to their additional resilience. They are built to better deal with fires, earthquakes, power outages, heatwaves, and a host of other issues. Multiple fuel sources give these facilities clinical resilience.
2.1 Clinical considerations
Patients and staff have a right to expect that engineering systems and equipment will be designed, installed, operated, and maintained to standards that will enable them to function efficiently, reliably, and safely. The unique nature of healthcare premises, and dependency of patients on the provision of effective and efficient engineering services, requires that engineering systems must be resilient to maintain the continuity of health services and ensure the ongoing safety of patients, visitors, and staff. Any modifications to these systems therefore need to be carefully planned and implemented to avoid unexpected isolations.
2.2 Energy consumption in hospitals
Hospitals are very energy dense buildings. The average energy density of a hospital in Victoria is 1.4 GJ/m2 per year [1]. To put that in perspective, a 5 star premium grade commercial office building in Melbourne would be around 0.35 GJ/m², making the hospitals around four times more energy dense.
It has been observed that the energy consumption in hospitals remains relatively consistent across different facilities, with a nearly equal split between gas and electricity (48% vs 52%) [1]. While detailed research is limited primarily to Victorian hospitals, other research has shown that this figure appears consistent, with figures from hospitals around the world showing similar consumption trends [2].
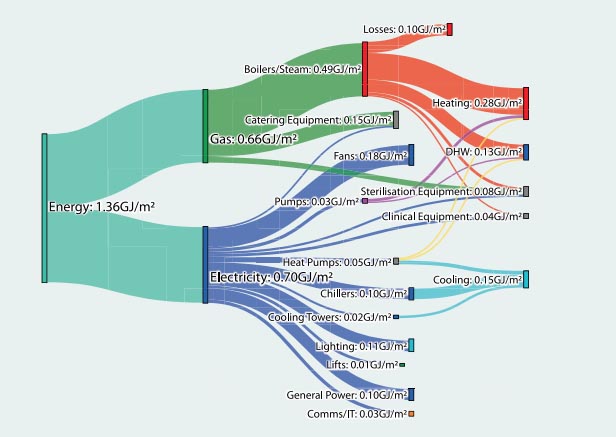
Gas consumption analysis reveals that 74% is attributed to heating boilers and steam generation equipment, 20% is utilised for catering purposes, and 7% is directly allocated to sterile services departments. On the other hand, electricity consumption is categorised into lighting, general power, equipment, and HVAC systems, which aligns with expected divisions. Notably, HVAC systems emerge as the primary energy consumer, constituting approximately 65% of the total energy consumed by hospitals. This significant proportion can be attributed to the substantial ventilation requirements and associated air-treatment processes employed in healthcare facilities. A further breakdown of the systems to their final use is shown in figure 1 below.
2.3 Typical gas–fired systems
Figure 1 indicates the main systems consuming natural gas in a hospital are domestic hot water (DHW), heating (via heating hot water (HHW)), steam generation and catering equipment. These systems and their criticality to a hospital’s workings are described in the following sections.
Figure 1 indicates the main systems consuming natural gas in a hospital are domestic hot water (DHW), heating (via heating hot water (HHW)), steam generation and catering equipment. These systems and their criticality to a hospital’s workings are described in the following sections.
2.3.1 Domestic hot water system
The domestic hot water system in a hospital is designed to supply heated water for non-medical purposes, including handwashing, bathing, and cleaning. The system typically comprises a water heating unit, such as a boiler or water heater, along with storage capabilities to meet the hospital’s demand. Its primary objective is to ensure a consistent supply of hot water throughout the facility, promoting hygiene and comfort for staff, patients, and visitors.
For inpatient facilities, especially aged care, these systems are critical to ensure the comfort of patients. Further, hand hygiene is an important aspect of infection control, and so warm water for hand washing is imperative.
2.3.2 Heating hot water system
The heating hot water system plays a critical role in maintaining optimal temperatures within the hospital premises. This system facilitates the delivery of hot water required by mechanical plant to treat supply air.
A central heating boiler is commonly employed to raise the water temperature, which delivers heat to the airside systems via heat exchangers. The heating hot water system ensures a comfortable environment for patients, staff, and visitors during colder seasons. As with the DHW system, heating plays a crucial part of inpatient comfort and safety.
2.3.3 Catering
The catering system within a hospital encompasses all processes related to food preparation, cooking, and distribution to cater to the dietary requirements of patients, staff, and visitors. Food preparation requires a large amount of energy in a relatively small space, and so gas–fired equipment has been a preference of catering professionals since it was invented.
2.3.4 Steam generation
The steam system in a hospital serves vital functions in medical and sterilisation applications. Steam is extensively utilised for autoclaving equipment, sterilising surgical instruments, and creating a sterile environment in operating rooms. The system typically incorporates a steam generator or boiler, steam distribution piping, and pressure control mechanisms. By heating water to its boiling point and transferring the resulting vapour, the steam system plays a pivotal role in maintaining infection control protocols and ensuring patient and healthcare provider safety.
3. Environmental considerations
One of the key drivers for electrification is the environmental impact. Burning fewer fossil fuels is beneficial in reducing the effect of global warming. This is, of course, if the electricity being used in lieu of burning natural gas isn’t created using more polluting fossil fuels than natural gas. Unfortunately, in many areas of Australia this is currently the case.
3.1 Grid power source
In almost all states and territories in Australia (with the exception of South Australia and Tasmania), the carbon intensity of grid electricity is relatively high when compared to much of the rest of the world. In 2021, the average carbon intensity from electricity generation in Australia was 526.88 grams of equivalent carbon dioxide per kilowatt hours (CO2-e/kWh) [3]. The reason behind this figure being higher relatively than other high-GDP countries is the amount of brown coal burned to produce electricity.
This figure is trending down (even with increasing population) as coal-fired power stations are being decommissioned and more of the grid is being supplied by renewable sources. However, this still has a long way to go to catch up to the likes of Western Europe [4].
Comparatively, figures published in February 2023 state that a kilowatt hour from natural gas has emissions equivalent to 184.33 gCO2-e/kWh [5]. This means that in some circumstances, it is more environmentally friendly to burn natural gas than it is to use an electrical alternative.
Many government entities have committed to sourcing all of their electricity from renewable sources in the near future. For example, the Victorian government has pledged all electricity used in government operations will be 100 per cent powered from renewable sources by 2025 [6]. In 2022, 35.9% of Australia’s electricity generated was from renewable sources [7], so clearly this solution isn’t possible for all.
3.2 Renewable energy sources
Electrification and renewable energy are closely intertwined. If the electricity being produced is from renewable sources, electricity as a fuel source is almost always preferred. If the power can be created locally, this is even more beneficial because there are fewer losses associated with transmission.
Unfortunately, many large hospitals, especially in more densely populated areas, do not have the luxury of space for on-site renewables. Hospital roofs are often burdened with critical engineering services and lack adequate space for installing renewable energy systems like solar panels. Additionally, rooftop space is often allocated for helipads and other vital infrastructure components. These limitations restrict the capacity for installing renewable energy systems on hospital rooftops, further complicating the transition to all-electric systems.
4. Demand implications
4.1 Equivalent electrical systems
Natural gas has been used for a long time, primarily to create heat, because it is so energy dense and abundant. The systems described in section 1.3 (DHW, HHW, steam and catering) are all using various forms of heat to provide a service in the hospital. These systems are vital to the operation of a hospital, and so for natural gas to be removed, alternative technologies need to be employed to maintain the function. Replacing gas–fired systems with alternative technologies has implications for the infrastructure of the hospital.
4.1.1 Heat pumps
The most efficient technology to replace natural gas alternatives for the DHW and HHW systems are heat pumps. A heat pump is a thermodynamic device that utilises the principles of refrigeration to transfer heat from one location to another. It operates by extracting heat energy from a low-temperature source, such as ambient air, groundwater, or the earth, and then amplifies and delivers it to a higher-temperature space.
By utilising the refrigeration cycle, a heat pump can efficiently transfer heat in both heating and cooling modes. In heating mode, the heat pump extracts heat from the external environment and transfers it indoors, providing warmth. In cooling mode, the process is reversed, with heat being removed from indoors and expelled outdoors. For the purposes of DHW and HHW systems, we are primarily concerned with the heating ability of these devices, because cooling is typically already electrically based.
When considering system replacements, it is worth noting that these systems have different requirements. A DHW system has load spikes typically early in the morning and generally consistently throughout the day after this. A DHW system also has to be watermarked, as the water is being consumed and supplied for contact by humans. The design temperature of a traditional DHW system is 60°C.
Note: a watermarked heat exchanger can be added to the system, but this adds additional energy losses to the system.
Conversely, an HHW system is a closed-loop system, meaning that the energy is being taken from the water to supply heat, but is not having to heat incoming domestic cold water (DCW). The HHW is supplied to the field typically around 80°C and returns at 60°C. There are variances in this, but the difference in temperature (ΔT) is a reasonably consistently 20°C historically.
This distinction is important because the different temperatures mean that the coefficient of performance (CoP) of the two systems can vary significantly. In Melbourne design conditions for example, at 3°C ambient, the CoP of a heat pump supplying 60°C DHW is around 3.5. For an HHW system at 80°C, the CoP is closer to 2, i.e., much less efficient in the use of energy to create heat.
In a new HHW system that is designed with lower flow and return temperatures, the CoP can increase; however, for retrofit works this is rarely an opportunity, because it requires replacement of additional equipment that is not designed to cater for the lower temperatures.
Finally, heat pumps require significantly more physical space than a traditional boiler or calorifier. This adds further complications when considering retrofit works to existing hospitals. Space is already a premium, so additional plant space requirements often means compromise elsewhere.
4.1.2 Catering Equipment
Due to the high temperatures required and instant demand, refrigerant–based systems are not an option for an alternative to gas–fired cooking. This means cooking through electrical means is reliant on either resistive elements or induction to produce heat. Both of these technologies have a (near) 1 to 1 conversion for electrical energy in to heat energy delivered, unlike refrigerant based systems described above which can achieve more better ratios (1 to 4 and above). In short, this means replacing gas–fired cooking with electric only requires significantly more power.
4.1.3 Steam generation
As with catering equipment, the high temperatures required to produce steam mean that resistive elements are the only viable method for creating steam from an electrical input. Again, this results in higher power requirements for the equivalent system.
4.2 Infrastructure implications
The removal of natural gas from a hospital necessitates an increase in electrical demand due to the continued requirement of various systems within the facility.
To accurately estimate the corresponding electrical load per system, it is necessary to analyse the gas demand and break it down according to the specific systems and their respective demands. For instance, the heating portion of boilers can be replaced by heat pumps. By considering factors such as boiler losses and the coefficient of performance of typical heat pumps, the electrical demand required to replace the gas-fired system can be determined.
It is crucial to assess each system individually, because the electrical-to-heat energy conversion efficiency varies depending on the specific technology employed. By summing up the electrical demands of these systems, an approximate increase of 40–50% in electrical energy consumption can be calculated. It is important to note that these figures may vary on a case-by-case basis, but they generally align with the observed trend.
Table 1 below gives an overview of a practical example of this. The data used in this analysis was obtained from a Melbourne hospital and Melbourne design conditions.
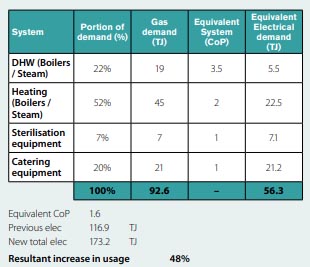
In terms of maximum demand, it is essential to consider the existing peak load conditions and the timing of the additional load. When these figures are evaluated using an IES (Integrated Environmental Solutions) model, it indicates that the increased maximum demand also sees an approximate 50% increase. However, there is a shift in the peak demand occurrence from summer to winter due to the changes in the heating system.
It is evident that transitioning away from natural gas in a hospital setting introduces a significant increase in electrical demand. Understanding the specific requirements of each system and assessing the corresponding electrical-to-heat energy conversion efficiencies are crucial for accurately estimating the overall demand. By incorporating these factors into the analysis, hospitals can better plan and manage the increased electrical load while ensuring a reliable and sustainable energy supply.
Around Australia, the grid (particularly in the CBD areas) is currently facing capacity challenges, necessitating infrastructure upgrades for various projects, even for minor increases in demand. Achieving a 25% increase per site, particularly for existing category 1 hospitals, presents a significant undertaking.
In the case of our example hospital, the maximum demand would rise from 9.5MVA to approximately 13.5MVA. This would entail multiple and costly substation upgrades, requiring careful planning to ensure uninterrupted power supply. Sustained offline status of one of the mains supplies poses a considerable risk to clinical services, warranting a robust management strategy. Additionally, it is important to consider that there may be additional infrastructure upgrades required beyond the hospital site, and determining the party responsible for funding these upgrades becomes a critical question.
5. Conclusion
In conclusion, the electrification of buildings, particularly hospitals, is a pressing and complex issue. Hospitals are not like other commercial buildings – their primary purpose is patient care, which necessitates a unique approach to energy use. While efforts to “green” hospitals are commendable, such initiatives must always consider the unique demands and functions of healthcare facilities.
Given that hospitals are not low-energy consumers, and factoring in the high-energy density they possess, the move towards complete electrification presents significant challenges. The current capacity of Australia’s grid and the high CO2 emissions per kWh, particularly in Victoria and New South Wales, also exacerbate these challenges. Moreover, removing natural gas supplies for hospitals will result in increased electrical demand, and potentially impact local infrastructure.
Future endeavours must consider the unique nature of hospital energy use, such as multiple fuel sources for clinical resilience and the role of HVAC systems in energy consumption. Any alterations or regulations to these energy systems must ensure that they continue to function efficiently, reliably, and safely.
In the light of these considerations, the way forward is not to rush into full electrification of critical facilities, but to continue striving for a balance between green energy initiatives and the paramount goal of providing high-quality patient care. Efforts should be directed towards reducing energy consumption where possible, without compromising patient care. Furthermore, improvements to the grid, the exploration of diverse and multiple energy sources, and careful planning for hospital energy use are all necessary components of the road ahead.
Lastly, the impact on local infrastructure must be considered when planning for an increase in electrical demand. Upgrades to substations and an assurance of continuity in power supply are paramount to ensure that clinical services are not disrupted. As such, electrification of hospitals is not merely an engineering challenge, but also a socio-economic one, requiring a thoughtful and measured approach. It’s an endeavour that goes beyond merely “going green” – it’s about maintaining an environment where health and well-being are prioritised.
References
[1] Victorian Department of Health 2012, ‘Energy use and carbon emissions in a major metropolitan hospital’. Energy break-up in health services, accessed 19 June 2023
[3] Granwal, L 2022.; “Emissions intensity from electricity generation in Australia 2012-2021”, accessed 19 June 2023,
[4] electricitymap.tmrow.co. (n.d.). Live 24/7 CO2 emissions of electricity consumption. [online]
[5] Victorian Department of Climate Change, Energy, The Environment and Water 2023, ‘Australian National Greenhouse Accounts Factors’. Climate Change, accessed 19 June 2023
[6] Whole of Victorian Government 2021, ‘Cutting Victoria’s Emissions 2021–2025’. Climate Change, accessed 19 June 2023
[7] Clean Energy Council 2023 ‘Clean Energy Australia Report 2023’
This article appears in Ecolibrium’s August-September 2023 edition
View the archive of previous editions





Latest edition
See everything from the latest edition of Ecolibrium, AIRAH’s official journal.