Meeting IAQ requirements in a South Australian canteen environment: reverse cycle versus indirect evaporative cooling



Abstract
Poor indoor air quality is increasingly recognised as a hidden health risk, driving respiratory problems, exacerbating chronic disease, and accelerating the transmission of airborne infections. This study evaluated whether indirect evaporative cooling (EC) systems can improve indoor air quality (IAQ) and infection control risks compared with conventional reverse cycle (RC) systems. Experiments were conducted in a South Australian canteen during the summer season, selected as a high-occupancy environment with consistent cooking and occupancy conditions across treatments. Occupancy was manually counted with either an indirect evaporative cooling or reverse cycle system operating. The reverse-cycle system consisted of two split systems, neither of which supplied outdoor air – a common scenario in these types of buildings. Indoor air quality parameters such as CO₂, PM₂.₅, PM₁₀, Total Volatile Organic Compounds (TVOC), temperature, air exchange rate and humidity were measured continuously during operational hours (9am–5pm), capturing peak activity with occupancy sensors.
This project demonstrated that an indirect evaporative cooling system achieved a high air change rate (ACH/h) (13.05/h) and recorded significantly reduced pollutant concentrations in the space compared to when it was operating under reverse cycle conditions. CO₂, PM (particulate matter), and TVOC levels were all statistically significantly lower with the indirect evaporative cooling compared with the reverse cycle (p<0.01), while relative humidity remained within the optimal 40–60% range for infection control and thermal comfort. Spearman’s correlation showed a strong positive relationship between CO₂ and PM and TVOC levels, indicating accumulation at a rate inversely correlated to ventilation effectiveness. Indirect evaporative cooling performance achieved key targets set out under ASHRAE Standard 241, met thresholds in the IAQ blueprint, and the Lancet Commission’s ventilation benchmarks. These results support indirect evaporative cooling as a viable ventilation option for achieving health-based IAQ standards within the built environment, particularly in climate zones conducive to its operation.
Introduction
Standards and regulations
Clean indoor air has now been recognised as a fundamental human right, with the World Health Organization calling for ventilation to be treated as central to protecting public health (Allen, 2024). The COVID-19 pandemic further underscored the urgent need for buildings designed with infection control in mind, where ventilation and air cleaning act as primary barriers to airborne disease transmission (Chen & Li, 2024; Heydari & Abbasianjahromi, 2024). Yet, despite decades of IAQ research, most building codes still prioritise thermal comfort over infection risk reduction (Allen, 2024; ASHRAE, 2020; Zaniboni & Albatici, 2022).
In response, recent international efforts, including The Lancet COVID-19 Commission (The Lancet COVID-19 Commission Task Force on Safe Work, 2022), the IAQ blueprint published in Science (Morawska, 2024 #17195) and ASHRAE Standard 241 have shifted the focus to health-based and performance‑driven ventilation standards (Azimi, 2022; Jones et al., 2025; Morawska et al., 2024). These documents collectively establish higher minimum ventilation requirements and performance standards to safeguard against airborne transmission in all built environments.
Health effects of contaminants in air
Indoor air contaminants can present a significant human health risk. The partial pressure of carbon dioxide (pCO₂) is the measure of CO₂ within arterial or venous blood (Messina & Patrick, 2022). It serves as a physiological marker of sufficient alveolar ventilation within the lungs (Messina & Patrick, 2022). Carbon dioxide (CO₂) concentration, typically reported in parts per million (ppm), reflects the amount of CO₂ present in indoor air.
In indoor environments, elevated CO₂ concentrations can lead to corresponding increases in pCO₂ in the blood through inhalation, linking environmental exposure to physiological response (Azuma et al., 2018). Exposure to ambient CO₂ values which result in pCO₂ levels >600ppm has been shown to lead to “sick-building syndrome”. This is a situation in which the occupants of a building experience acute health- or comfort-related effects that seem to be linked directly to the time spent in the building, resulting in irritation, fatigue, anxiety, headaches, poor cognitive performance and sleep apnoea, and linked to elevated pCO₂ in blood (Du et al., 2020; Guyenet & Bayliss, 2015; Iwayama et al., 2025; Joshi, 2008; Seppänen et al., 1999; Tsai et al., 2012).
However, the role of CO₂ at these concentrations remains debated, with many studies indicating that CO₂ primarily acts as an indicator of ventilation effectiveness and co ‑accumulated bioeffluents rather than a direct causal agent of adverse health effects (Mendell et al., 2021; Persily, 2015; Wargocki et al., 2020). Improvements in occupant outcomes have been observed with increased ventilation rates (e.g. 10–20L/s per person), often at CO₂ concentrations below 800ppm, suggesting that ventilation ‑related factors rather than CO₂ alone may drive these effects. Existing studies on the effect of elevated CO₂ on human health focus on the effects of exposure to acute CO₂ levels and/or cognitive responses to elevated indoor CO₂ levels (Du et al., 2020; Karnauskas et al., 2020).
The effects of human exposure to elevated CO₂ levels have been mostly assessed in terms of physiological and cognitive levels (Jacobson et al., 2019). Higher CO₂ concentrations (>1,200–1,600ppm) have been more consistently associated with direct physiological effects, although thresholds remain uncertain. However, subtle changes may operate through disruptions of human proteome functions under chronic exposure to elevated CO₂ levels (C. M. Duarte et al., 2020). This has been proposed as a hypothesis rather than confirmed evidence, suggesting a potential mechanistic pathway under prolonged exposure to elevated concentrations. The effects of human exposure to elevated CO₂ on the proteome can elicit broad systemic impacts, but is an area that requires further research (Carlos M. Duarte et al., 2020).
New evidence suggests that volatile organic compounds (VOCs) such as aromatic and aliphatic compounds in the indoor home environment are associated with an increased risk of asthma and asthma-like symptoms (including wheeze) in adults (Paterson et al., 2021). Particulate matter (PM), regardless of particle size, can have negative health impacts, including increasing risk of cardiovascular and respiratory morbidity. Indoor PM specifically has been associated with increased respiratory symptoms (Simoni, 2002).
A study conducted in 421 houses in northern‑central Italy showed a positive correlation between indoor PM2.5 exposure and the presence of bronchitis and asthmatic symptoms, especially during the winter season (Simoni, 2002). A study conducted in Oslo, Norway, showed that indoor suspended PM contained a large amount of potential allergen carriers (soot particles <1μm) (Ormstad, 2000). The presence of organic pollutants together with these allergens or endotoxin may exert a proinflammatory effect, leading to the exacerbation of allergic diseases such as asthma (Leung et al., 2002; Ormstad, 2000).
Mechanisms by which PM exerts adverse respiratory effects by acting as a possible adjuvant have been reviewed previously (Bernstein et al., 2004; Diaz-Sanchez et al., 1997). Indoor PM may carry toxic pollutants and reaction products into the airways, generating oxidative stress (Ormstad, 2000). Many organic chemicals (e.g. polycyclic aromatic hydrocarbons and quinones) associated with ambient PM are redox active and have been shown to induce proinflammatory responses through the generation of oxidative stress (Leem et al., 2005; Li et al., 2003). Finally, reactive compounds, such as free radicals and organic compounds, generated from the interactions between indoor PM, O3, or NO2 can also have proinflammatory effects (DiazSanchez et al., 1997; Mølhave et al., 2005; Strand et al., 1997; Tunnicliffe et al., 1994).
Reverse cycle versus evaporative cooling
It is timely to examine the comparative benefits of indirect evaporative cooling (IDEC) and reverse cycle (RC) split systems for IAQ and infection control against this backdrop of IAQ developments, as these systems fundamentally differ in their mode of air delivery, with IDEC supplying 100% outdoor air and RC split systems primarily recirculating indoor air.
IDEC systems, by design, deliver 100% outdoor air without recirculation, aligning closely with health-focused standards such as the NonInfectious Air Delivery Rate (NADR) defined by the Lancet Commission and the Equivalent Clean Airflow Rate (ECAi) introduced by ASHRAE 241, where EC contributes through direct provision of outdoor air rather than relying on equivalent clean air from filtration or air cleaning technologies. By contrast, reverse cycle systems remain heavily dependent on recirculated air. This study explores how these two approaches to cooling differ in their capacity to deliver clean, safe, and sustainable indoor air.
Evaporative cooling achieves air cooling through the evaporation of water, typically by passing air through a wetted medium or water spray, where the evaporating water absorbs its latent heat of vaporisation from the air, resulting in a reduction in air temperature. This is an adiabatic saturation mechanism in which evaporating water absorbs its heat of evaporation from the flowing air, thus cooling it (Chijioke, 2017; Khalid, 2008; Watt & Brown, 1997). The effectiveness of this process is strongly dependent on ambient conditions, as dry and warm air, with lower absolute humidity, has a greater capacity to absorb water vapour, making evaporative cooling more effective in drier climatic regions (Chijioke, 2017; Khalid, 2008).
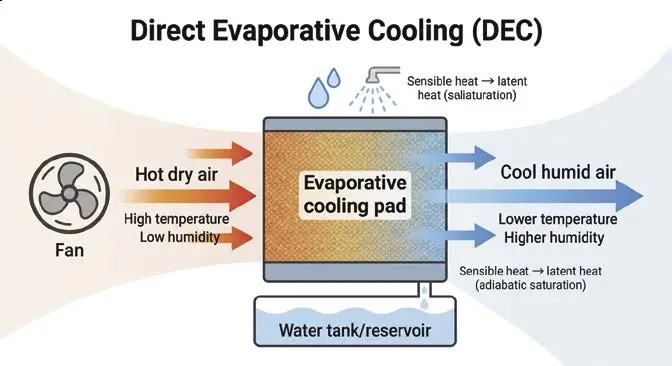
Figure 1: Direct evaporative cooling system
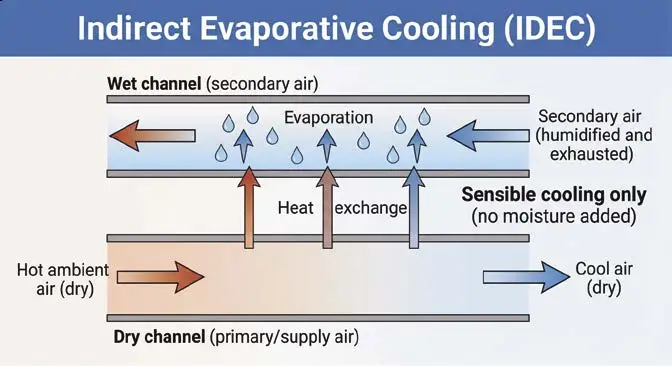
Figure 2: Indirect evaporative cooling system
Types of evaporative cooling system
Evaporative cooling systems are classified into three types:
- Direct evaporative cooling system (DEC)
- Indirect evaporative cooling system (IDEC)
- Multistage evaporative cooling system.
Direct evaporative cooling (DEC) systems operate by passing hot ambient air through a wetted medium. Figure 1 shows the schematic of the DEC system. Heat from the air is absorbed by the water as it evaporates from the wetting medium, resulting in simultaneous cooling and humidification of the supply air. The minimum achievable temperature is the wet-bulb temperature of the incoming air (Abbouda & Almuhanna, 2012; Camargo et al., 2005; Chijioke, 2017; Watt & Brown, 1997). This heat absorption reduces the temperature and increases the humidity of the air due to evaporation of water (Chijioke, 2017). In DEC, the temperature of the air cannot be cooled below the wet-bulb temperature of the air (Chijioke, 2017; Kapilan et al., 2023). This type of cooling is suitable for dry and hot climates (Kapilan et al., 2023).
In contrast, an indirect evaporative cooling system (IDEC) differs from the direct type because the temperature of the air is reduced without adding any moisture (Kapilan et al., 2023; Riangvilaikul & Kumar, 2010), an advantage over conventional DEC systems. Indirect evaporative cooling systems utilise a heat exchanger to transfer cooling from a secondary, moisture-laden airstream to a primary supply airstream without direct contact (Duan et al., 2012; Maheshwari et al., 2001). The secondary cooled moist air is released outside, while the conditioned supply air remains dry. The heat exchanger in an IDEC system can reduce the temperature below the wet-bulb temperature, making it more suitable for indoor environments where humidity control is required (Gómez et al., 2010; Hsu et al., 1989). Figure 2 shows the schematic of the IDEC system.
The system performance remains strongly climate dependent. Since evaporative cooling relies on the air’s capacity to absorb moisture, it is most effective in hot, dry, and temperate climates, including arid, semi-arid, and Mediterranean regions (Al-Helal, 2001; Costelloe & Finn, 2003; Guan et al., 2015).
Methods
Study setting
This case study was conducted in a South Australian canteen (volume 552m³) (Figure 3), during the summer season, which was characterised by warm-to‑hot ambient temperatures and relatively low humidity. The experiment aimed to compare indoor air quality under two distinct ventilation conditions: a reverse cycle (RC) split system and an indirect evaporative cooling (IDEC) system.
The RC condition used two reverse cycle air conditioners. Each unit had a cooling capacity of 8–9kW and a heating capacity of 9–11.5kW under standard conditions (DB/WB 27°C/19°C for cooling; 20°C/15°C for heating). The rated power input was 3.4kW, with a current draw of 14.5A. While the space may warrant additional split systems based on typical sizing, practical constraints such as infrastructure limitations and budget often restrict the number that can be installed in real-world settings. These units recirculated air within the test space and provided an air change rate of approximately 2.3–2.5 ACH per unit. The reverse cycle units were standard wall‑mounted split systems that recirculate indoor air and do not introduce outdoor air. Accordingly, the reported air change rates (2.3–2.5 ACH per unit) represent internal air movement rather than true ventilation, and do not contribute to fresh air exchange. This equated to over 23 minutes to condition the facility’s air volume, reflecting the limitations of recirculating systems in delivering fresh air exchanges.
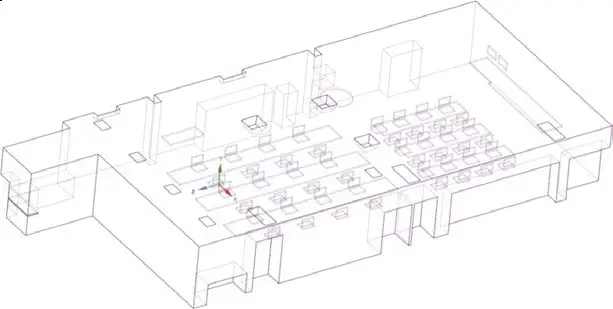
Figure 3: Schematic representation of canteen showing room size, EC vents, RC systems, table arrangement, and exhaust vents. This figure illustrates a ~552m³ room with the EC system (CW-X2) delivering 7,200m³/h of 100% outdoor air (13 ACH, 4.6-minute air change), indirect evaporative cooling (IDEC) vents, two RC systems (~5.6L/s per person, 2.3–2.5 ACH), and table arrangement for ~50 occupants.
In contrast, the indirect evaporative cooling system (CW-X2) supplied 7,200m³/h of 100% outdoor air, achieving an air change rate of 13.05/h and conditioning the full air volume within 4.6 minutes. Airflow was measured at 2,400L/s, with a cooling capacity of 25kW. This system was equipped with a MERV 8 filter, providing moderate filtration efficiency by capturing larger airborne particles such as dust, pollen, and mould spores. The use of MERV 8 filtration is consistent with ASHRAE 62.1 requirements for non‑healthcare facilities, including offices, schools, and food preparation areas, where the priority is both equipment protection and removal of coarse particulate matter.
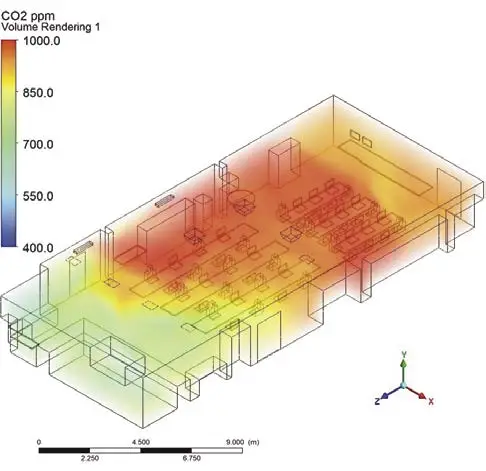
Figure 4: Schematic representation of CO₂ levels in a canteen with reverse cycle split systems. This figure depicts CO₂ concentrations across a roughly 552m³ room, where two reverse cycle split systems provide estimated 2.3–2.5 air changes per hour, resulting in CO₂ concentrations of 850–1,000ppm.
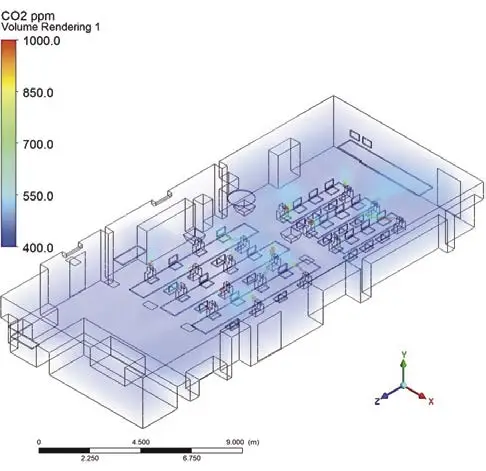
Figure 5: Schematic representation of CO₂ levels in the same canteen with indirect evaporative cooling systems. This figure depicts CO₂ concentrations across the 552m³ room, where the indirect evaporative cooling system (CW-X2) delivers 7,200m³/h of outdoor air (13.05 ACH, 4.6-minute air change), maintaining CO₂ at 450ppm.
Figures 4 and 5 show the computational fluid dynamics (CFD) modelling of the canteen facility using ANSYS 2024. CO₂ concentration is shown at 1.3m above the floor, representing the breathing zone. Dark blue areas indicate lower concentrations (<500ppm), while yellow to red areas denote elevated levels (>800ppm). Under indirect evaporative cooling, a larger blue zone is visible, reflecting greater dilution of occupant‑generated CO₂ compared with reverse cycle operation. Localised yellow-red areas highlight zones of weaker airflow where CO₂ accumulates. Computational fluid dynamics simulations were conducted using ANSYS Fluent (ANSYS 2024 R2).
Measurements
IAQ parameters CO₂, TVOCs, PM₂.₅ and PM₁₀, temperature (T) and relative humidity (RH), were continuously monitored using Milesight multisensors integrated with LoRaWAN technology for real-time data transmission. Sensors were positioned at 1.3m above the floor to reflect the breathing zone relevant to seated and standing occupants. To minimise interference from the EC supply vents and return ducts, all sensors were placed at least 1.3m away from direct airflow pathways (shown in Figure 3). This ensured accurate measurement of CO₂ concentrations as a proxy for ventilation effectiveness and air quality within the occupied zone. CO₂ levels were measured using a nondispersive infrared (NDIR) sensor with a range of 400–5,000ppm, an accuracy of ±30ppm plus 3% of the reading, and a resolution of 1ppm. TVOC concentrations were detected using a metal oxide (MOX) MEMS sensor with a range of 1.00–5.00 IAQ rating units and a resolution of 0.01. PM₂.₅ and PM₁₀ were monitored via laser scattering with a range of 0–1,000μg/m³
and a resolution of 1μg/m³. Temperature and humidity were recorded using digital MEMS sensors with accuracies of ±0.2°C and ±2% RH, respectively. This setup enabled high-resolution, low‑power environmental monitoring under field conditions as described in Table 1.
Table 1 presents sensor specifications used for monitoring indoor environmental parameters. Data were continuously recorded and summarised as median values with interquartile ranges (IQR) for the occupied period (9am–5pm).
Measurements were conducted across three experimental replicate days for each treatment, where each replicate represented a full-day measurement under matched operational conditions, undertaken on alternate days over a two‑week period when outdoor temperatures consistently exceeded 30°C. This ensured participants remained comfortable under either RC or EC operation. Trials were performed only on fully sunny, hot days to minimise weather variability, with external conditions (temperature, relative humidity, and wind speed/direction) monitored and days selected to ensure comparable ranges across treatments. Five sensors were placed on individual tables and operated from 9am–5pm. Prior to data collection, each system was run until the room was fully conditioned: approximately 25 minutes for RC, consistent with its air change rate, and 4.5 minutes for EC. Measurements commenced only after complete air conditioning had been achieved, with data during system stabilisation excluded from analysis.
Table 1. Sensor specifications

Statistical analysis
Non-parametric analysis was conducted using Kruskal-Wallis tests to evaluate treatment effects on indoor air quality parameters, and Spearman’s rank correlation coefficient (rho) was used to assess correlations between CO₂ and PM2.5, PM10, and TVOC variables using SPSS. A significance level of p<0.05 was applied.
Carbon dioxide
EC systems maintained significantly lower indoor CO₂ levels than the RC systems (Kruskal‑Wallis H = 22.96, p<0.001), with narrower interquartile ranges indicating stable dilution of occupant-generated CO₂. RC treated spaces exhibited higher and more variable concentrations, suggesting reduced ventilation efficacy (Figure 6.1). These findings indicate improved ventilation performance under indirect evaporative cooling conditions.
PM₂.₅ and PM₁₀
Fine and coarse particle concentrations were higher under RC conditions in this study setting. Indirect evaporative cooling systems significantly reduced indoor PM₂.₅ (Kruskal‑Wallis H = 7.91, p = 0.005) and PM₁₀ (Kruskal-Wallis H = 8.15, p = 0.004) levels, likely due to higher outdoor air exchange and better dilution of indoor sources (Figures 6.2 and 6.3).
The lower concentrations observed under indirect evaporative cooling therefore indicate reduced occupant exposure to particle-related risks.
TVOC
Total volatile organic compounds levels were lower in the EC-treated space (Kruskal‑Wallis H = 9.00, p = 0.003) (Figure 6.4). The RC‑treated space exhibited higher variability and transient peak concentrations exceeding 3ppm, retained in the analysis and reflected in boxplot distributions (median and interquartile range), rather than excluded as statistical outliers. These peaks likely represent short-duration emission events (e.g. cooking or occupant activities), as data were quality‑checked and no evidence of instrument artefacts was identified, potentially due to off-gassing from indoor materials and limited fresh air intake. Elevated VOC exposure is associated with eye and airway irritation, headaches, and reduced wellbeing (Norbäck et al., 2017). Lower and more stable concentrations under EC indicate reduced occupant exposure.
Temperature and relative humidity
EC systems were associated with slightly lower but more stable indoor temperatures (Kruskal-Wallis H = 4.19, p = 0.041) (Figure 6.5), although a wider interquartile range indicates greater variability under EC conditions.
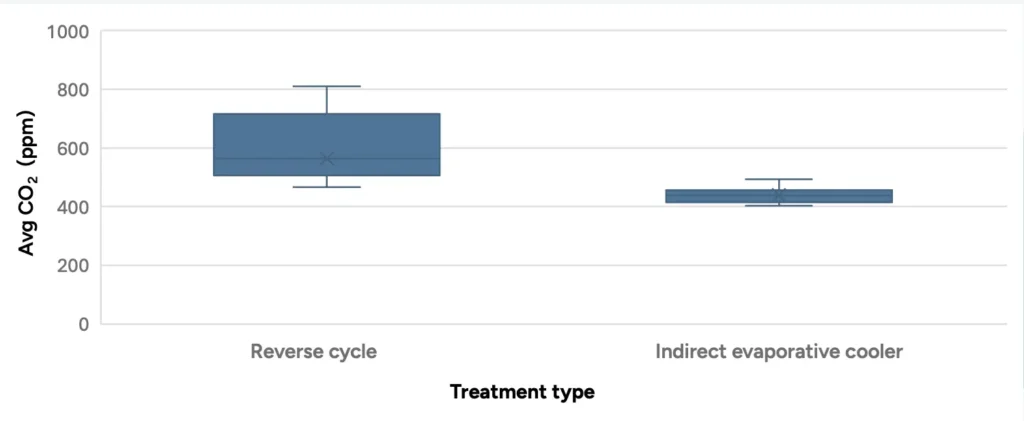
Figure 6.1: Boxplot showing average indoor CO₂ concentration (ppm) under RC split and indirect EC treatments. A statistically significant difference was observed (Kruskal-Wallis H = 22.96, p<0.001).
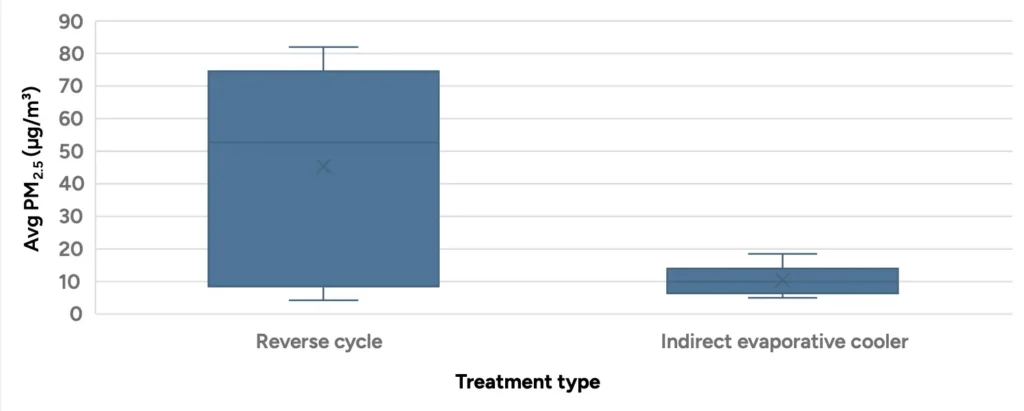
Figure 6.2: Boxplot comparing PM₂.₅ concentrations (μg/m³) under RC and indirect EC systems. EC treatment resulted in significantly lower PM₂.₅ levels (Kruskal-Wallis H = 7.91, p = 0.005)
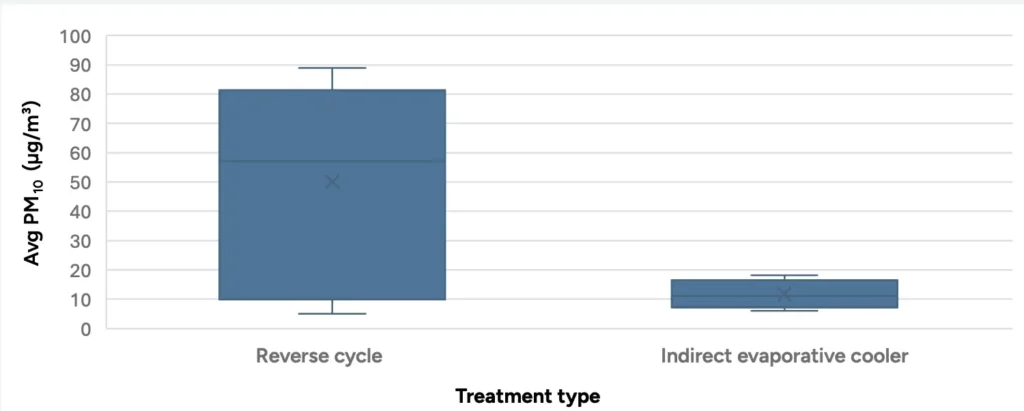
Figure 6.3: Boxplot comparing PM₁₀ concentrations (μg/m³) under RC and EC treatments. EC significantly reduced PM₁₀ levels compared to RC (Kruskal-Wallis H = 8.15, p = 0.004).
The lower concentrations observed under indirect evaporative cooling therefore indicate reduced occupant exposure to particle-related risks.
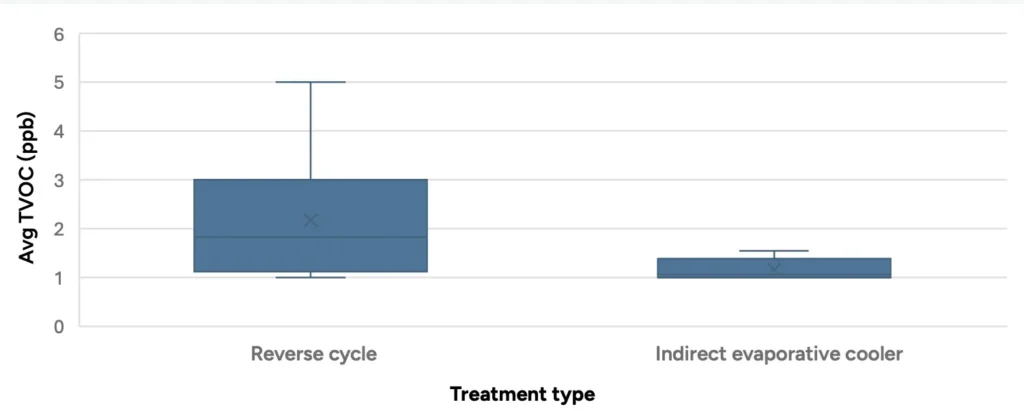
Figure 6.4: Boxplot showing TVOC concentrations (ppm) under RC and EC treatments. EC significantly reduced TVOC levels (Kruskal-Wallis H = 9.00, p = 0.003), suggesting better control of indoor gaseous pollutants.
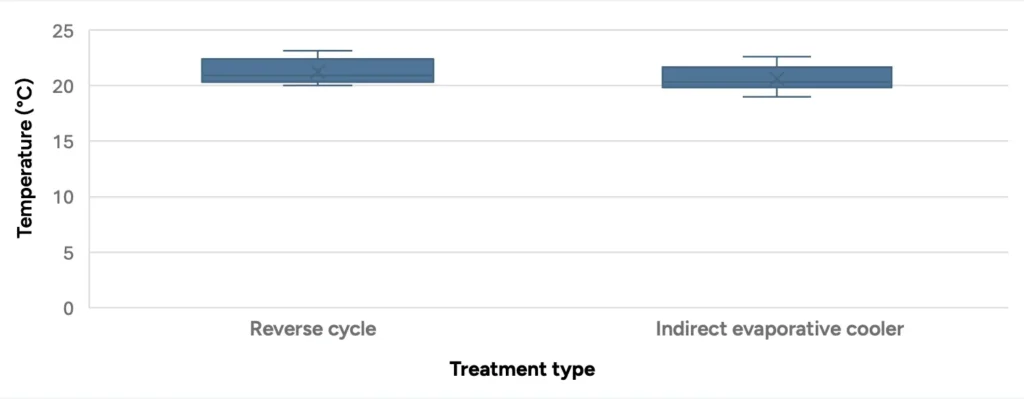
Figure 6.5: Boxplot of indoor temperature under RC and EC systems. A small but statistically significant difference was observed (Kruskal-Wallis H = 4.19, p = 0.041), with RC resulting in slightly higher temperatures.
Relative humidity was significantly higher and more variable in indirect evaporative cooling space, consistent with the humidifying nature of indirect evaporative cooling (Figure 6.6). Relative humidity influences aerosol dynamics, where higher levels can shorten aerosol suspension time and reduce airborne persistence; however, maintaining indoor humidity below approximately 60% is generally recommended, as excessive humidity may promote microbial and mould growth.
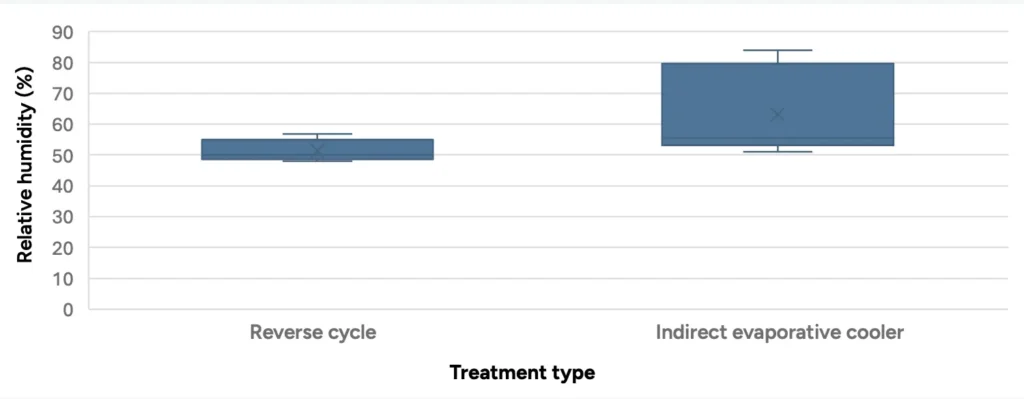
Figure 6.6: Boxplot of indoor relative humidity across treatments. EC significantly increased humidity levels compared to RC systems (Kruskal-Wallis H = 15.03, p<0.001).
Summary of findings
The results showed significantly lower CO₂, PM₂.₅, PM₁₀, and TVOC concentrations under EC compared to RC treatment as described in Table 2.
Table 2. Median comparison between RC and IDEC
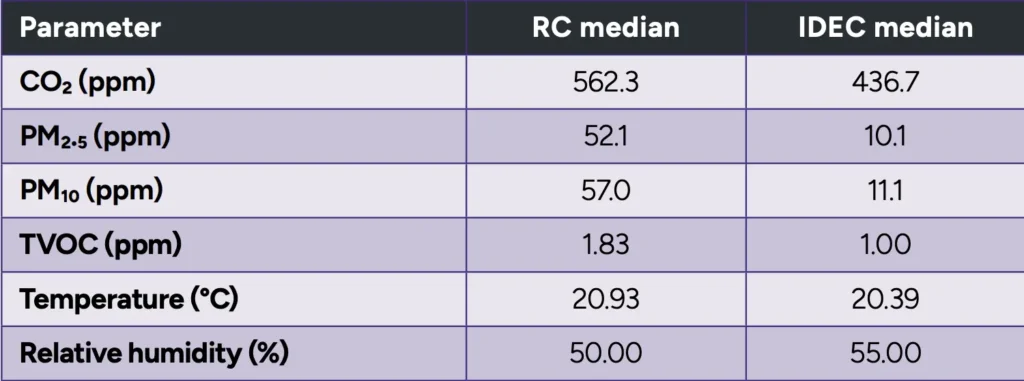
Table 2 presents the median values for indoor environmental parameters under the RC and indirect EC conditions. Values were derived from non-parametric analysis and are reported alongside Kruskal-Wallis test statistics, with indirect EC consistently associated with lower pollutant concentrations and higher relative humidity compared to RC operation. Median CO₂ concentrations were markedly lower under indirect EC (450ppm) than RC (650ppm), with a Kruskal-Wallis H value of 22.96 (p<0.001). PM concentrations were also significantly reduced under indirect EC: PM₂.₅ dropped from 55µg/m³ (reverse cycle) to 10 µg/m³, and PM₁₀ concentrations reduced from 70µg/m³ to 15µg/m³ (both p<0.01). Similarly, TVOC values were lower with indirect EC (1.1ppm) compared to RC (2.5 ppm, p = 0.003). RH was significantly higher under indirect evaporative cooling (60% vs 50%, p<0.001), supporting occupant comfort and respiratory health. Outdoor data confirmed warm, dry ambient conditions, where increasing RH is beneficial. Evidence indicates infection risk is lowest at 40–60% RH, with low humidity increasing aerosol generation and airway susceptibility, while moderate humidity improves airway function and reduces viral viability (Wolkoff, 2024). Accordingly, the increase in RH observed under indirect evaporative cooling aligns with this optimal range under dry conditions, supporting both thermal comfort and potential reductions in airborne infection risk. Where ambient humidity increases, complementary control strategies, such as hybrid or desiccant-assisted systems, may be applied to maintain RH within this optimal band while preserving ventilation effectiveness. Overall, the indirect EC system provided better IAQ (Kapilan et al., 2023).
Experimental controls
Occupancy was manually counted and verified using IR sensors, with comparable occupancy patterns and activity levels maintained across treatments. Cooking practices and operational schedules were consistent between experimental days. External conditions (temperature, relative humidity, and wind) were monitored, and trials were conducted under similar hot-weather conditions. Measurements were performed over the same time period (9am–5pm), with data collected only after system stabilisation.
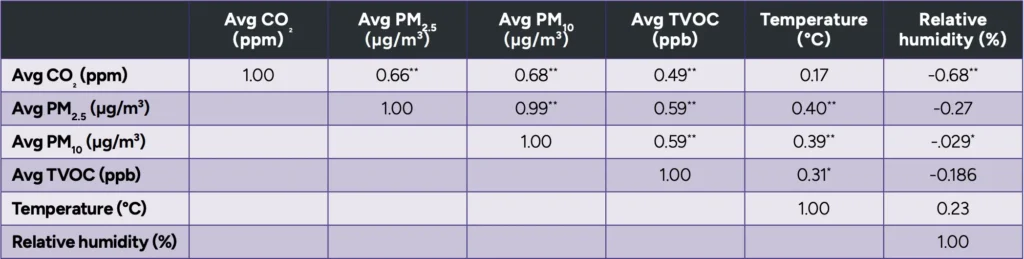
Table 3. Spearman correlation matrix.
Spearman’s correlation analysis
Spearman’s correlation coefficient is a non‑parametric measure of the strength and direction of a monotonic relationship between two variables, calculated using ranked data and appropriate for non-normally distributed datasets. Spearman’s correlation coefficient describes how strongly two variables change together, based on their ranked values, and is suitable for non-normally distributed data. Spearman’s correlation analysis revealed a strong, statistically significant positive relationship between CO₂ and PM. CO₂ with PM₂.₅ (rho = 0.656, p < 0.001) and CO₂ with PM₁₀ (rho = 0.677, p < 0.001), as well as with TVOC (rho = 0.489, p = 0.002) as detailed in Table 3.
Spearman’s correlation analysis revealed a strong, statistically significant positive relationship between CO₂ and PM. CO₂ with PM₂.₅ (rho = 0.656, p < 0.001) and CO₂ with PM₁₀ (rho = 0.677, p < 0.001), as well as with TVOC (rho = 0.489, p = 0.002) as detailed in Table 3. Table 3 presents strong positive correlations were observed between CO₂, PM₂.₅, PM₁₀, and TVOC, indicating coaccumulation under shared conditions such as occupancy and limited ventilation. Relative humidity showed a moderate negative correlation with CO₂, while temperature exhibited weak associations with other variables. These findings indicate that temporal concentrations of indoor pollutants correlate strongly, suggesting potential shared causes such as human occupancy, ventilation conditions, or air exchange dynamics.
The pattern is consistent with indoor environments using RC systems, where limited fresh air exchange may contribute to the co-accumulation of exhaled gases, particulates, and volatile compounds.
Discussion
This study provides empirical evidence that indirect evaporative cooling systems can align with the IAQ blueprint (Science, 2024), ASHRAE Standard 241 (Jones et al., 2025), and Lancet NADR in a canteen setting in conducive climate zones.
The EC system delivered 7,200m³/h of 100% outdoor air, achieving 13 ACH in a ~552 m³ space, with a 4.6-minute air change time. Assuming a default 50-person occupancy under ASHRAE 241, this yields an ECAi of 40L/s per person, exceeding the 30L/s per person target for a canteen and supporting Infection Risk Management Mode (IRMM) requirements for a ≤0.1% hourly infection probability (Jones et al., 2025). The RC systems, limited to ~5.6L/s per person (2–5 ACH), aligned with ASHRAE 62.1 (Ventilation for Acceptable Indoor Air Quality), but not IRMM. The RC systems met the IAQ blueprint CO₂ target but did not meet the PM₂.₅ or ventilation requirements. Indirect evaporative cooling systems improved CO₂, PM₂.₅ and TVOC levels compared to the RC systems, meeting IAQ blueprint targets for CO₂ and PM₂.₅ (Science, 2024) and satisfying the Lancet NADR ventilation benchmark for infection control (Allen Joseph, 2016), resulting in comparatively better IAQ outcomes under indirect evaporative cooling operation.
Ventilation dilutes virus-laden aerosols, reducing airborne transmission risk (Gilkeson et al., 2013). The 100% outdoor air delivered by indirect evaporative cooling aligns with NADR’s preference for minimising bioaerosol redistribution, achieving Re<1, which indicates that the effective reproduction number is below one, and transmission is not sustained within the space.
The 13 ACH delivered by indirect evaporative cooling exceeds the ventilation rates typically associated with ASHRAE 241 (4–12 ACH) and demonstrates the capacity to achieve high outdoor air exchange under the conditions tested. This level of ventilation supports applications in high-occupancy settings such as schools and gyms.
Limitations and suggestions for further research
This study was conducted in a single canteen under summer conditions in a warm, dry climate, and the findings should be interpreted within this context. System performance is climate-dependent, and outcomes may differ under more humid conditions. The reverse cycle system reflects the existing installed capacity, which may be lower than typically recommended for this space. Increasing capacity may improve thermal comfort, but would not improve ventilation or IAQ without additional outdoor air supply. Further research should assess both systems across different climates, occupancy levels, and configurations. Studies incorporating mechanical ventilation and humidity control would help identify where each system is most appropriate.
Conclusion
Indirect evaporative cooling provides a viable option to achieve emerging IAQ and infection control standards.
The indirect evaporative cooling system reduced CO₂, particulate matter, and volatile organic compounds through high outdoor air supply, resulting in concurrent changes across multiple IAQ parameters rather than isolated effects. While the use of outdoor air introduces a potential pathway for external pollutants, this can be addressed through the integration of filtration and additional air treatment where required, enabling application in polluted environments without compromising energy efficiency or overall IAQ performance. The potential for increased indoor particulate concentrations during bushfire events reflects the use of high outdoor air ventilation rather than an inherent limitation of indirect evaporative cooling and can be effectively mitigated through established integration of filtration and recirculation strategies. Its ability to deliver high outdoor airflow, reduce pollutant loads, and maintain relative humidity within ranges associated with occupant comfort and respiratory health, positions the technology as an alternative approach for healthy, lowcarbon buildings. Where ambient humidity increases, indirect evaporative cooling can be complemented with control strategies such as hybrid configurations or desiccant-assisted systems, enabling humidity to be reduced if required while maintaining high outdoor air delivery and ventilation effectiveness.
Indirect evaporative cooling systems offer a scientifically and policy-aligned solution to improving IAQ while mitigating airborne infection risk. In this study, both indirect evaporative cooling and reverse cycle systems met CO₂ targets; when assessed over the full sampling period; however, during peak occupancy periods (e.g. lunchtime), higher CO₂ concentrations and greater variability were observed under reverse cycle conditions compared to indirect evaporative cooling. By delivering 100% outdoor air without recirculation, indirect evaporative cooling achieved lower CO₂, PM₂.₅, PM₁₀, and TVOC concentrations than reverse cycle under the conditions tested in this canteen. These findings support the potential relevance of indirect evaporative cooling for health-focused ventilation in similar high-occupancy indoor environments.
Future work should further explore testing in other types of facilities and other climate zones, as well as reverse cycle systems that supply outdoor air. Evaluating additional outcome measures in indirect evaporative cooling ventilated environments may further inform long-term policy adoption.
Conflict of interest
The authors declare that Sonali Deshmukh and Patrick McCaffrey are employed by Seeley International, a manufacturer of direct and indirect evaporative air conditioning systems.
Funding
This research was supported by the Department of Education, Australian Government (project number 35318), Seeley International Pty Ltd and Flinders University as part of a National Industry PhD program.
Acknowledgements
S.D.,C.M., H.W., K.E.R. and P.Mc.C. designed and participated in the study. S.D. drafted and edited the manuscript. C.M. designed and simulated the CFD model. H.W., K.E.R. and P.Mc.C. reviewed and edited the manuscript. All authors have read and agree to the published version of the manuscript
References
- Abbouda, S. K., & Almuhanna, E. A. (2012). Improvement of evaporative cooling system efficiency in greenhouses. International Journal of Latest Trends in Agriculture & Food Sciences, 2(2), 83-89.
- Al-Helal, I. (2001). A survey study of cooling pads clogging problem for greenhouses and poultry buildings in central region of Saudi Arabia. Research Bulletin(105).
- Allen, J. G. (2024). Recommitting to Ventilation Standards for Healthy Indoor Air Quality. Am J Public Health, 114(10), 991-993. https://doi.org/10.2105/ajph.2024.307809
- ASHRAE. (2020). COVID-19 guidance for multifamily building owners/managers. merican Society of Heating, Refrigerating and Air-Conditioning Engineers. https://doi.org/https://www.ashrae.org/file%20library/technical%20resources/covid-19/covid-19-guidancefor-multifamily-building-owners_managers.pdf
- Azimi, P. K., Zahra; Jones, Emily; Allen, Joseph G.; Cao, Xiaodong; Cadet, Leslie R.; Chen, Yan; Corsi, Richard; Grier, Kelly; Levinson, Meira; Li, Yuguo; Macomber, John; Marr, Linsey; Michaels, David; Miller, Shelly; Morawska, Lidia; Munro, Alasdair; Pollock, Nira. (2022). Proposed Non-infectious Air Delivery Rates (NADR) for Reducing Exposure to Airborne Respiratory Infectious Diseases. https://covid19commission.org/safe-work-travel
- Azuma, K., Kagi, N., Yanagi, U., & Osawa, H. (2018). Effects of low-level inhalation exposure to carbon dioxide in indoor environments: A short review on human health and psychomotor performance. Environment International, 121, 51-56. https://doi.org/https://doi.org/10.1016/j.envint.2018.08.059
- Bernstein, J. A., Alexis, N., Barnes, C., Bernstein, I. L., Nel, A., Peden, D., Diaz-Sanchez, D., Tarlo, S. M., & Williams, P. B. (2004). Health effects of air pollution. Journal of allergy and clinical immunology, 114(5), 1116-1123.
- Camargo, J. R., Ebinuma, C. D., & Silveira, J. L. (2005). Experimental performance of a direct evaporative cooler operating during summer in a Brazilian city. International Journal of Refrigeration, 28(7), 1124-1132.
- Chen, T.-L., & Li, Y.-E. (2024). Building urban resilience: Lessons from the COVID-19 pandemic for future-proofing city infrastructure. Journal of Urban Management. https://doi.org/https://doi.org/10.1016/j.jum.2024.11.016
- Chijioke, O. V. (2017). Review on evaporative cooling systems. Greener Journal of Science, Engineering and Technological Research, 7(1), 1-20.
- Costelloe, B., & Finn, D. (2003). Indirect evaporative cooling potential in air–water systems in temperate climates. Energy and Buildings, 35(6), 573-591.
- Diaz-Sanchez, D., Tsien, A., Fleming, J., & Saxon, A. (1997). Combined diesel exhaust particulate and ragweed allergen challenge markedly enhances human in vivo nasal ragweed-specific IgE and skews cytokine production to a T helper cell 2-type pattern. Journal of immunology (Baltimore, Md.: 1950), 158(5), 2406-2413.
- Du, B., Tandoc, M. C., Mack, M. L., & Siegel, J. A. (2020). Indoor CO₂ concentrations and cognitive function: A critical review. Indoor Air, 30(6), 1067-1082.
- Duan, Z., Zhan, C., Zhang, X., Mustafa, M., Zhao, X., Alimohammadisagvand, B., & Hasan, A. (2012). Indirect evaporative cooling: Past, present and future potentials. Renewable and Sustainable Energy Reviews, 16(9), 6823-6850.
- Duarte, C. M., Jaremko, Ł., & Jaremko, M. (2020). Hypothesis: Potentially Systemic Impacts of Elevated CO₂ on the Human Proteome and Health [Hypothesis and Theory]. Frontiers in Public Health, Volume 8 – https://doi.org/10.3389/fpubh.2020.543322
- Duarte, C. M., Jaremko, Ł., & Jaremko, M. (2020). Hypothesis: Potentially Systemic Impacts of Elevated CO(2) on the Human Proteome and Health. Front Public Health, 8, 543322. https://doi.org/10.3389/fpubh.2020.543322
- Gómez, E. V., Martínez, F. R., & González, A. T. (2010). The phenomenon of evaporative cooling from a humid surface as an alternative method for air-conditioning. Journal homepage: www. IJEE. IEEFoundation. org, 1(1), 69-96.
- Guan, L., Bennett, M., & Bell, J. (2015). Evaluating the potential use of direct evaporative cooling in Australia. Energy and Buildings, 108, 185-194. https://doi.org/https://doi.org/10.1016/j.enbuild.2015.09.020
- Guyenet, P. G., & Bayliss, D. A. (2015). Neural control of breathing and CO₂ homeostasis. Neuron, 87(5), 946-961.
- Heydari, A., & Abbasianjahromi, H. (2024). Evaluating the resilience of residential buildings during a pandemic with a sustainable construction approach. Heliyon, 10(10), e31006. https://doi.org/https://doi.org/10.1016/j.heliyon.2024.e31006
- Hsu, S. T., Lavan, Z., & Worek, W. M. (1989). Optimization of wet-surface heat exchangers. Energy, 14(11), 757-770.
- Iwayama, R., Shimatani, K., Nakayama, Y., Takaguchi, K., Nakaoka, H., Suzuki, N., & Sakurai, K. (2025). The Relationship Between Ventilation and BuildingRelated Symptoms in Modern High-Performance Japanese Houses: A Cross-Sectional Study Using Building-Specification Data. Buildings, 15(17), 3013.
- Jacobson, T. A., Kler, J. S., Hernke, M. T., Braun, R. K., Meyer, K. C., & Funk, W. E. (2019). Direct human health risks of increased atmospheric carbon dioxide. Nature Sustainability, 2(8), 691-701.
- Jones, B., Iddon, C., Zaatari, M., Wargocki, P., & Bruns, R. (2025). Risk modeling for ASHRAE Standard 241 2023 – Control of infectious aerosols. Building and Environment, 283, 113318. https://doi.org/https://doi.org/10.1016/j.buildenv.2025.113318
- Joshi, S. M. (2008). The sick building syndrome. Indian J Occup Environ Med, 12(2), 61-64. https://doi.org/10.4103/0019-5278.43262
- Kapilan, N., Isloor, A. M., & Karinka, S. (2023). A comprehensive review on evaporative cooling systems. Results in Engineering, 18, 101059. https://doi.org/https://doi.org/10.1016/j.rineng.2023.101059
- Karnauskas, K. B., Miller, S. L., & Schapiro, A. C. (2020). Fossil fuel combustion is driving indoor CO₂ toward levels harmful to human cognition. GeoHealth, 4(5), e2019GH000237.
- Khalid, A. (2008). Experimental investigation and mathematical modelling of a low energy consuming hybrid desiccant cooling system for the hot and humid areas of Pakistan NED University of Engineering and Technology]. Karachi, Pakistan.
- Leem, J. H., Kim, J. H., Lee, K. H., Hong, Y. c., Lee, K. H., Kang, D., & Kwon, H. J. (2005). Asthma attack associated with oxidative stress by exposure to ETS and PAH. Journal of Asthma, 42(6), 463-467.
- Leung, T.-f., Lam, C. W., Chan, I. H., Li, A. M., Ha, G., Tang, N. L., & Fok, T.-f. (2002). Inhalant allergens as risk factors for the development and severity of mild-to-moderate asthma in Hong Kong Chinese children. Journal of Asthma, 39(4), 323-330.
- Li, N., Sioutas, C., Cho, A., Schmitz, D., Misra, C., Sempf, J., Wang, M., Oberley, T., Froines, J., & Nel, A. (2003). Ultrafine particulate pollutants induce oxidative stress and mitochondrial damage. Environmental Health Perspectives, 111(4), 455-460.
- Maheshwari, G., Al-Ragom, F., & Suri, R. (2001). Energy-saving potential of an indirect evaporative cooler. Applied Energy, 69(1), 69-76.
- Messina, Z., & Patrick, H. (2022). Partial pressure of carbon dioxide. In StatPearls [Internet]. StatPearls Publishing.
- Mølhave, L., Kjærgaard, S. K., Sigsgaard, T., & Lebowitz, M. (2005). Interaction between ozone and airborne particulate matter in office air. Indoor Air, 15(6).
- Morawska, L., Allen, J., Bahnfleth, W., Bennett, B., Bluyssen, P. M., Boerstra, A., Buonanno, G., Cao, J., Dancer, S. J., Floto, A., Franchimon, F., Greenhalgh, T., Haworth, C., Hogeling, J., Isaxon, C., Jimenez, J. L., Kennedy, A., Kumar, P., Kurnitski, J., . . . Yao, M. (2024). Mandating indoor air quality for public buildings. Science, 383(6690), 1418- https://doi.org/10.1126/science.adl0677
- Norbäck, D., Hashim, J. H., Hashim, Z., & Ali, F. (2017). Volatile organic compounds (VOC), formaldehyde and nitrogen dioxide (NO2) in schools in Johor Bahru, Malaysia: Associations with rhinitis, ocular, throat and dermal symptoms, headache and fatigue. Science of the Total Environment, 592, 153-160. https://doi.org/https://doi.org/10.1016/j.scitotenv.2017.02.215
- Ormstad, H. (2000). Suspended particulate matter in indoor air: adjuvants and allergen carriers. Toxicology, 152(1-3), 53-68.
- Paterson, C. A., Sharpe, R. A., Taylor, T., & Morrissey, K. (2021). Indoor PM2.5, VOCs and asthma outcomes: A systematic review in adults and their home environments. Environmental Research, 202, 111631. https://doi.org/https://doi.org/10.1016/j.envres.2021.111631
- Riangvilaikul, B., & Kumar, S. (2010). An experimental study of a novel dew point evaporative cooling system. Energy and Buildings, 42(5), 637-644. https://doi.org/https://doi.org/10.1016/j.enbuild.2009.10.034
- Seppänen, O., Fisk, W. J., & Mendell, M. J. (1999). Association of ventilation rates and CO₂ concentrations with health andother responses in commercial and institutional buildings. Indoor Air, 9(4), 226-252.
- Strand, V., Rak, S., Svartengren, M., & Bylin, G. (1997). Nitrogen dioxide exposure enhances asthmatic reaction to inhaled allergen in subjects with asthma. American journal of respiratory and critical care medicine, 155(3), 881-887.
- Tsai, D.-H., Lin, J.-S., & Chan, C.-C. (2012). Office workers’ sick building syndrome and indoor carbon dioxide concentrations. Journal of Occupational and Environmental Hygiene, 9(5), 345-351.
- Tunnicliffe, W., Burge, P., & Ayres, J. (1994). Effect of domestic concentrations of nitrogen dioxide on airway responses to inhaled allergen in asthmatic patients. The Lancet, 344(8939-8940), 1733-1736.
- Watt, J. R., & Brown, K. B. (1997). Evaporative air conditioning handbook. Chapman and Hall.
- Wolkoff, P. (2024). Indoor air humidity revisited: Impact on acute symptoms, work productivity, and risk of influenza and COVID-19 infection. International Journal of Hygiene and Environmental Health, 256, 114313. https://doi.org/https://doi.org/10.1016/j.ijheh.2023.114313
- Zaniboni, L., & Albatici, R. (2022). Natural and Mechanical Ventilation Concepts for Indoor Comfort and Well-Being with a Sustainable Design Perspective: A Systematic Review. Buildings, 12(11), 1983. https://www.mdpi.com/2075-5309/12/11/1983

This article appears in Ecolibrium’s Autumn 2026 edition
View the archive of previous editions





Latest edition
See everything from the latest edition of Ecolibrium, AIRAH’s official journal.